
Glaucoma

About Glaucoma
- About Glaucoma
- Pharmaceutical treatment of Glaucoma
- Glaucoma Laser Treatment
- Microinvasive Glaucoma Surgery (MIGS)
- Trabeculectomy and Glaucoma Drainage Devices
About Glaucoma
Dr Siempis’s practice offers specialised glaucoma services including diagnosis, monitoring and treatment of all types of glaucoma. The doctor’s approach is to treat each patient holistically while at the same time individualise the treatment according to their needs aiming to maintain the best possible vision and quality of life.
An one stop glaucoma diagnosis visit is available as the office is equipped with the latest diagnostic equipment like the iCare Compass® perimeter and colour fundus photo camera, an Optical Coherence Tomorgraphy scanner from Nidek (Retina Scan Duo ™ 2), Corneal Pachymetry (DGH Pachmate 2) and the innovative service of home tonometry (eye pressure measurement) with the iCare Home 2 device.
What is more, Dr Siempis offers access to the most effective, safe and up to date laser and surgical treatment options like Selective Laser Traceculoplasty, Microinvasive Glaucoma Surgery, Microinvasive Bleb Surgery as well as traditional glaucoma surgery in the form of Trabeculectomies and Glaucoma Drainage Device Implantation (Ahmed Glaucoma Valve, Baerveldt tube shunt and Paul tube).
What is glaucoma?
More specifically, most types of Glaucoma, like Primary Open Angle Glaucoma or Pseudoexfoliative Glaucoma or Primary Closed Angle Glaucoma, are associated with high intraocular pressure without any pain or change of vision and the patient can only develop symptoms when the disease has progressed to a more advanced stage.
Symptoms of Glaucoma include a change in vision in terms of quality, clarity, loss of peripheral field of vision or appearance of blind spots within the field of vision. Having said that, there are certain cases like the Acute Angle Closure Attack which cause dramatic symptoms like severe eye pain, headache, nausea and or vomiting. This is an ophthalmic emergency and urgent medical care should be sought.
Risk factors
At the same time, glaucoma is more common in people of African, Latin American or Asian Descent. As far as past medical history is concerned, having a history of diabetes, hypertension, sleep apnea, migraines or nocturnal hypotension also increase the risk of developing glaucoma. The same applies for patients who are on long term steroid medications of any form. Finally, previous eye injuries, inflammation of the eye, increased myopia or hypermetropia are also risk factors for glaucoma.
Can glaucoma be prevented?
Regular eye exams are also recommended for patients with sleep apnoea and nocturnal hypotension. In such cases, the ophthalmologist will liaise with the respective physician to address these issues. Last but no least, protecting our eye from any type of injury is also very important. Leading a healthy lifestyle, regular exercises and eating green vegetables and fruit are also of help when it comes to maintaining good vision.
Types of Glaucoma
Another significant categorisation is based on the status of the drainage angle of the eye with some glaucomas being what we call “Open Angle” glaucoma and some being “Closed Angle” glaucoma. The differentiation is done doing a special clinical examination called gonioscopy and with supplementary imaging modalities like the Anterior Segment Optical Coherence Tomography - OCT which is available in Dr Siempis’s office and UBM - Ultrasound Biomicroscopy.
The most common type of glaucoma on a worldwide basis that affects 2.5% of the global population is Primary Open Angle Glaucoma (POAG) where the drainage angle of the eye is open but there is impaired drainage of the aqueous fluid that is produced within the eye. This prevalence of POAG increases to 10% in patients over the age of 75. On the other hand, Primary Angle Closure Glaucoma is less common (0.4% in people over the age of 40 and 0.95% in people over the age of 70 in European populations) but it is more aggressive and more commonly associated with extensive visual field loss in not adequately treated due to significant fluctuations in the intraocular pressure.
How is the diagnosis made and what does the consultation include?
Taking a detailed history is paramount followed by a comprehensive and thorough clinical examination with ancillary testing like Visual Field Testing, andOptical Coherence Tomography (OCT) as this approach minimises the chances of missing a diagnosis of glaucoma.
Dr Siempis has an expertise in glaucoma diagnosis and management being a fellowship trained glaucoma specialist by one of the leading Glaucoma and Advanced Anterior Segment Surgeons, Dr Ike Ahmed.
At the initial consultation, the doctor will obtain a detailed clinical history, identify risk factors for developing glaucoma and then perform the following tests:
- Comprehensive eye examination using a slit lamp.
- Goldmann Applanation Tonometry
- Gonioscopy-Central Corneal Thickness (Pachymetry)
- Visual field testing using the iCare Compass automated perimetry with active retinal tracking
- Optical Coherence Tomography of the optic nerve and macula as well as the anterior segment
- Colour Fundus Photography
Based on the results of the above tests, the doctor will recommend whether treatment is needed and formulate a treatment plan to manage this chronic disease in a stepwise approach.
If there is already a diagnosis of glaucoma, then the aforementioned tests are adjusted accordingly on an individual basis.
**It is worth noting that the pupils will be dilated except in cases of angle closure glaucoma and for this reason, it is advisable that the patient has somebody to accompany them to the office.
How often should one get checked for glaucoma?
The interval between the regular eye exams should be further individualised based on the presence of the risk factors described in the above subsections. People with positive family history fro glaucoma or history of diabetes should get annual eye check ups over the age of 40.
Unfortunately, sometimes there can be a delay in diagnosing glaucoma or starting the appropriate treatment and this can have an adverse effect in the long term outcome of the disease. This is why it is advisable to seek expert glaucoma care if there is a strong suspicion of glaucoma or a diagnosis of glaucoma.


Pharmaceutical treatment of Glaucoma
Medical treatment in the form of eye drops and less often in the form of pills, is the most commonly used treatment for glaucoma. The advantages of medical treatment are that it is effective in the majority of patients, it can be initiated at any time, it is non invasive and overall is safer compared to glaucoma surgery in terms of any potential serious complications.
In the last few years though, Ophthalmologists started to acknowledge that the use of multiple glaucoma drops and especially the ones with preservatives can have a negative impact on the ocular surface. At the same times, glaucoma drops and tablets have their own topical and systemic side effects that are described in detail below.
Selective Laser Trabeculoplasty and Microinvasive Gaucoma Surgery offer a way of bridging the gap between medical treatment and the traditional glaucoma surgeries of Trabeculectomy and Glaucoma Drainage Device mplantation.
In the sections below, the main types of the most commonly used drops for the treatment of glaucoma are described.
Prostaglandin Analogues
Prostaglandin analogues achieve on average a 30% reduction in Intraocular Pressure (IOP) and this makes this type of glaucoma eye drops more effective compared to the other categories. There are also fixed dose combination drops of Prostaglandin Analogues with B-blockers.
Overall, prostaglandin analogues are very well tolerated. They can cause mild redness of the conjunctiva (the lining of the eye). Other side effects include the non reversible change in the iris colour (tends to become darker due to increase melanin production), the thickening of the eyelashes as well as changes in the pigmentation of the skin around the eye and the fat of the orbits (eye sockets). The later are partially reversible upon cessation of the eye drops.
B-blockers
They have a very low rate of ocular side effects but they are commonly associated with systemic side effects. The main ones are Bronchospasm (that can cause shortness of breath) and Bradycardia (slow heart rate). These side effects are usually seen in patients that already have a history of lung diseases like asthma or COPD or cardiac disease. For this reason, it is very important to obtain a thorough medical history and explain to the patient of the potential side effects. It is also advisable to ask patients to close their eyelids for a minute or so after the instillation of the drops in order to reduce the amount of systemic absorption. Finally, another disadvantage of b-blockers is that they can lose their efficacy with time (tachyphylaxis).
Topical Carbonic Anhydrase Inhibitors (CAIs)
Topical CAIs reduce the eye pressure (IOP) by 16% to 24% so they are not as effective as monotherapy. They reduce IOP by reducing the amount of fluid (aqueous) produced within the eye. They are usually reserved as second or third line treatment when the IOP reduction achieved by Prostaglandin Analogues or B-blockers is not adequate. Their efficacy in terms of IOP reduction increases when they are used as fixed combinations with B-blockers (Cosopt or Azarga) or A2 adrenergic agonists (Simbrinza).
Overall, they are well tolerated and the most common side effects are a burning sensation upon instillation of the drops or exacerbation of dry eye. If there is a pre-existing dysfunction of the corneal endothelium (like Fuch's Endothelial Corneal Dystrophy), they can be associated with worsening of corneal oedema. Finally, few patients might experience headaches, changes in their taste or paraesthesias of their hands or feet.
Alpha 2- adrenergic agonists
Apraclonidine is usually used for a short period of time, commonly before or after glaucoma laser treatment as it associated with increased side effects like dry mouth or nose, mild eyelid retraction, topical allergic reactions or even drowsiness in older ages.
Brimonidine on the other hand is much well tolerated and is commonly used as a 3rd of 4th line treatment due to increased rates of allergic conjunctivitis. It is also available in fixed dose formulations with Timolol (Combigan) or Brinzolanide (Simbrinza). As far as other side effects are concerned, Brimonidine just like Apraclonidine can cause low blood pressure or drowsiness as it crosses the blood brain barrier and it must not be used in infants under the age of 6 months.
Sympathomimetics
Their usage has gradually declined over the years as more efficacious and better tolerated drops have emerged like the ones that are described in the previous section. The increased rate of side effects causes poor tolerance and common side effects include blurring of vision, headaches, cataract formation and in rare cases retinal detachment.
Systemic Carbonic Anhydrase Inhibitors
The most common side effects are increased diuresis (frequency of urination), paraesthesias at the fingers and toes, metallic taste, fatigue, gastrointenstinal upset, electrocyte imbalance and rarely changes in the blood cells (red blood cells and platelets) or severe skin reactions like Stevens Johnson Syndrome and Toxic Epidermal Necrolysis.
Glaucoma Laser Treatment
There are various types of glaucoma laser treatments and their indications vary. These include YAG peripheral iridotomy, Selective Laser Trabeculoplasty, Transcleral Cyclophotocoagulation with the use of Cyclodiode Laser and Endoscopic Cyclophotocoagulation that can be combined with cataract surgery and Microinvasive Glaucoma Surgery.
Dr Siempis has significant experience in all of the aforementioned types of laser. In the subsections below there is a summary of the indications, efficacy and safety profile for all types of glaucoma laser.
YAG Peripheral Iridotomy
In some cases, the crystalline lens pushes forward against the pupillary margin (the edge of the what we perceive as the black part in the centre of the eye) and this impairs the flow of aqueous between the anterior and posterior chamber causing what we call a pupillary block. When there is an increased relative pupillary block and in some cases an absolute pupillary block, the peripheral iris bows forward towards the drainage angle, occludes it and causes increased eye pressure (Intraocular Pressure - IOP). In such cases doing a peripheral iridotomy can facilitate the flow of aqueous between the two chambers of the eye and improve the IOP.
The main indications for doing a YAG peripheral iridotomy are an acute angle closure attack, some cases of chronic angle closure glaucoma and prophylactically in patients where there is an increased risk of developing high IOPs due to the narrowing of the drainage network of the eye with some additional risk factors (Primary Angle Closure Suspects - Plus).
With the advent of new imaging modalities such as the Anterior Segment Optical Coherence Tomography (ASOCT) that the office is equipped with, the understanding of the underlying mechanisms of angle closure has improved in the recent years. As a result, the need for a YAG peripheral iridotomy for each patient can be determined based on the underlying angle closure mechanism. At the same time, large Randomised Control Trials (RCTs), like the EAGLE and ZAP studies have given us new insights as to when Clear Lens Extraction is superior to a YAG peripheral iridotomy in patients with angle closure and also when YAG peripheral iridotomy has a protective effect in asymptomatic patients with a narrow drainage network within the eye (Primary Angle Closure Suspects).
What does the procedure involve?
The laser treatment is done in the office and does not require any preparation from a patient’s point of view. The eye is anaesthetised with the use of topical anaesthetic drops and and at the same time eye pressure lowering drops are instilled (Pilocarpine 2% and Apraclonidine 1%) in preparation for the laser. With the use of a special lens that rests on the surface of the eye (Abraham iridectomy lens), the laser is focused on the iris and a small number of laser shots are applied that create a tiny hole in the iris, the colour part of the eye. The patient might feel a small tingling or biting sensation for a few seconds.
Postoperative care and potential side effects:
After the laser treatment, steroid eye drops are prescribed for one week in order to control any postoperative inflammation and a follow up check takes places 4 weeks after the laser in order to check the eye pressure and the anatomy of the anterior chamber.
With respect to potential side effects, they are not very common, they are treatable and usually transient. Tese include micro bleed from the iris, a spike in the IOP, prolonged inflammation or glare.
Selective Laser Trabeculoplasty (SLT)
Selective Laser Trabeculoplasty (STL) has changed significantly the way that Primary Angle Closure Glaucoma (POAG) and Ocular Hypertension (OHT) are managed. It is now considered a first line treatment for patients that are newly diagnosed with POAG and OHT. At the same time, it can also be used in patients who already have a diagnosis of POAG and are using glaucoma eye drops and in selected cases it can either further lower the eye pressure (Intraocular Pressure -IOP) or reduce the number of glaucoma eye drops to achieve the target pressure. It is also effective in selected cases of Pseudoexfoliative Glaucoma, Pigment Dispersion Glaucoma, Steroid related glaucoma and even Juvenile Open Angle Glaucoma. Through Dr Siempis’s office, there is access to SLT that is done at St Luke’s Hospital.
The laser used is called YAG laser (Q-switched, frequency-doubled 532 nm neodymium:yttrium-aluminum-garnet laser) and the laser shots are of short duration and very low energy. There is selective uptake of the laser from the trabecular meshwork, which is the main outflow system of the aqueous fluid (the fluid that is constantly produced wihtin the eye), and this in essence causes changes in the consistency of a trabecular meshwork and increases its ability to drain aqueous fluid more effectively thereby reducing the IOP.
Scientific evidence supporting the use of SLT/ Efficacy and safety profile:
SLT has been extensively studied in numerous studies and trials. The LiGHT trial is the largest Randomised Control Trial (RCT) to date comparing the use of glaucoma eye drops with SLT as the first line tratment in patients newly diagnosed with Ocular Hypertension or Primary Open Angle Glaucoma (mild to moderate severity).
The results of this study show that at 36 months, 95% of the patients in the SLT group were within the target pressure and 3/4 of these patients achieved this on no glaucoma drops. At the same time, fewer patients had visual field deterioration and needed cataract or glaucoma surgery compared to the ones using glaucoma drops. The study also confirmed the excellent safety profile of SLT.
At 72 months, SLT continued to be superior to glaucoma drops. As a result, the National Institute for Health and Care Excellence (NICE) in the United Kingdome now recommends SLT as the first line treatment in patients with Primary Open Angle Glaucoma (mild to moderate) or Ocular Hypertension.
The duration of action of SLT varies but one application is usually effective in controlling the IOP for 1 or 2 years. It can be safely repeated if needed. It takes approximately 6 weeks to see its effect on the IOP. It might not be as successful in eyes that are already on maximum glaucoma eye drops and inadequate IOP control.
What does the procedure involve?
The laser treatment takes place as an outpatient appointment. It does not require any preparation from a patient’s point of view. The eye is anaesthetised with the use of topical anaesthetic drops and at the same time eye pressure lowering drops are instilled (Pilocarpine 2% and Apraclonidine 1%) in preparation for the laser. With the use of a special lens that rests on the surface of the eye (Latina SLT gonio lenss), the laser beam is focused on the trabecular meshwork and on average 100 shots are applied at an area covering 360 degrees of the trabecular meshwork. The patient does not feel any pain except some pressure like feeling from the lens that rests on the surface of the eye.
Postoperative care and potential side effects:
An IOP check is done 1 hour after the procedure and the patient can then go home and return immediately to their daily activities. The vision might be blurred for a day ar so and mild sensitivity to light might be present but these symptoms are transient. The IOP is then rechecked 6 weeks after the laser treatment. Potential side effects include a transient IOP spike, inflammation (iritis), microbleeding within the front part of the eye and corneal haze. These are uncommon and treatable with medical treatment.
Transcleral Cyclodiode Laser
Cyclophotocoagulation is used in glaucoma cases in which the Intraocular Pressure (IOP) has been very difficult to control with medical or surgical treatment or in cases where surgical treatment has a high risk of failure. Such cases include neovascular, congenital or related to Penetrating Keratoplasty glaucomas. It is also used in glaucoma cases where there is limited visual potential. Generally speaking it is reserved for later stages in the course of the disease.
Its mechanism of action lies in the destruction of the epithelial cells of the ciliary body that are responsible for aqueous fluid production thereby reducing the amount of aqueous fluid produced and the IOP. The lasers that are used for Cyclophotocoagulation are primarily Diode type lasers.
What does the procedure involve?
The laser treatment usually takes place in a Day Surgery Unit as it requires deep local anaesthesia usually in the form of a retrobulbar or peribulbar block. As a result, anaesthetic cover is usually advised in case of a reaction to the anaesthetic.
Postoperative care and potential side effects:
The laser treatment does not require any preparation from a patient’s point of view and the patient can return home the same day without any restrictions. After the procedure, frequent instillation of steroid drops is warranted for 6-8 weeks. An IOP check is needed on the first post-operative day, first post-operative week and then at the 4th post operative week in order to see the full effect of the laser.
Side effects are common and these include macular oedema that can lead to reduction of the central vision, intraocular inflammation or haemorrhage, low or high IOP and in some cases phthisis of the eye
Endoscopic Cyclophotocoagulation
Endoscopic cyclophotocoagulation is a variation of transcleral cyclophotocoagulation. Both work similarly with respect to how they achieve IOP reduction by destroying the epithelial cells of the ciliary body that are responsible for aqueous production.
The main difference is that Endoscopic Cyclophotocoagulation achieves this in a more controlled way as there is direct visualisation of the ciliary processes and the laser can be titrated based on its effect on the ciliary processes. Hence, the safety profile of Endoscopic Cyclophotocoagulation is superior compared to that of Transcleral Cyclophotocoagulation. For this reason, it is not considered a treatment of last resort for difficult to treat glaucomas but can be actually used earlier in the disease process usually in combination with cataract surgery or Microinvasive Glaucoma Surgery.
It can also be used in selected cases of angle closure glaucoma that undergo cataract surgery in order to improve the anatomy of the angle by remodelling the ciliary processes. This is particularly useful in cases of Plateau Iris Syndrome.
Postoperative care and potential side effects:
The postoperative care is similar to that of cataract surgery as it is almost always done in combination with it. Potential side effects include pronounced intraocular inflammation, transient IOP spike, intraocular bleeding, macular oedema and rarely loss of vision due to an infection or a serious haemorrhage
Microinvasive Glaucoma Surgery (MIGS)
Microinvasive Glaucoma Surgery (MIGS) along with the newer term of Microinvasive Bleb Surgery (MIBS) have changed radically the way that most types of glaucoma are managed nowadays.
These surgeries do not replace the traditional glaucoma surgeries of Trabeculectomy and Glaucoma Drainage Device Implantation. They do offer though a safe way of intervening earlier at the course of the disease and potentially achieving better long term outcomes in terms of visual field loss.
Glaucoma is a lifelong disease and as a result a lifelong plan is needed in order to prevent the patient from losing functional vision over the course of their lifetime. Medical treatment, despite the fact that it is effective in a significant proportion of glaucoma cases, it might not be enough on its own to stabilise the visual field loss.
MIGS and MIBS surgeries can bridge the gap that existed until recently between medical treatment and the more involved and risky traditional glaucoma surgery.
Dr Thomas Siempis has performed hundreds of MIGS and MIBS procedures and is a certified Surgeon of the iStent® , Hydrus® and Preserflo® glaucoma implants. During his surgical fellowship in the University of Toronto, he worked as an associate of Dr Ike Ahmed who is a world class Glaucoma and Anterior Segment Surgeon and was voted as the most influential Ophthalmologist in the world for 2024.
Dr Ike Ahmed is considered the “father” of Microinvasive Glaucoma Surgery (MIGS) as he has designed, developed and conducted clinical trials for a significant number of MIGS surgeries and devices. Thousands of MIGS cases are performed every year at Prism Eye Institute and Credit Valley Hospital in Canada where Dr Siempis worked for a year during his fellowships, with unparalleled access to the newest techniques and devices . For this reason, Dr Siempis solidified his surgical skills on MIGS and MIBS while gaining significant experience in the patient selection, pre-operative assessment as well as post-operative management of glaucoma patients undergoing such procedures.
What is more, Dr Siempis always audits his clinical results in order to confirm the safety and efficacy of the aforementioned procedures as these are already described in various clinical trials.
If a patient is eligible for MIGS or MIBS, the doctor will guide the patient through the process and recommend the best type of treatment on an individual basis.
What do the terms MIGS and MIBS refer to?
The aforementioned surgeries are very efficacious with regard to the lowering of the Intraocular Pressure (IOP) that is the only modifiable risk factor for the progression of glaucoma for now, but have a significant rate of postoperative complications and their longevity is limited by the natural tendency of the body for healing. This drive for healing usually manifests with the build up of scar tissue around these surgeries and this gradually diminishes their effectiveness. This results in reserving this cases for later in the disease process but at that time, results can be suboptimal. Microinvasive Glaucoma Surgery και Microinvasive Bleb Surgery are able to bridge the gap between medical treatment and the “bigger” glaucoma operation through their excellent safety profile and good efficacy. As a result, glaucoma specialists are now able to offer surgery at an earlier stage which means that there are more chances of altering the course of the disease and also improve the patients’ quality of life by reducing the number of glaucoma drops.
The term MIGS is actually an umbrella term that includes any type of glaucoma surgery that has the following characteristics:
-Ab-interno technique
-Minimally invasive
-Excellent safety and efficacy profile
-Faster recovery compared to traditional glaucoma surgery
MIGS surgeries include among others devices like the iStent® and Hydrus®, the technique GATT (Goniscopy Assisted Transluminal Trabeculotomy) and goniotomies with the use of a Kahook Dual Blade (KDB). iStent® implantation, the GATT technique as well as the KDB goniotomy are available in Greece and offered by Dr Siempis. In the future, the Hydrus® is expected to launch in Greece.
MIGS have either a neutral or synergistic action with cataract surgery which is in contrast to Bleb based surgeries whose efficacy is reduced when combined with cataract surgery.
The term MIBS (Microinvasive Bleb Surgery) on the other hand is reserved for Bleb based surgeries which are similar to trabeculectmy in terms of their efficacy but come with a more favourable safety profile. MIBS surgeries include the Xen Gel® Stent και Preserflo® SIBS Microshunt. Το Xen ®Gel Stent is available for use in Greece and the Preserflo® is expected to launch at some point too.
iStent®
The iStent® implants have a maximum diameter of 360 microns and are made of non magnetic titanium. They are compatible with MRI scanners up to 3 Tesla. To date, there are 3 types iStent® available. The first two are called the G1 and G2W iStents and are available for use in Europe whereas the third generation of iStents is called the iStent® infinite and is available for now only in the United States and Canada.
When is this surgery recommended?
Over 1 million iStents® have been implanted to date across the world and this reflects the excellent safety profile of the device that is combined with good efficacy data in selected glaucoma patients. Aside from Primary Open Angle Glaucoma patients, the iStent can be used for other types of glaucoma such as Pseudoexfoliative Glaucoma, Primary Angle Closure Glaucoma without peripheral anterior synechiae as well as in selected cases of Ocular Hypertension. In the majority of cases, it is combined with cataract surgery and this is one of the main advantages of this type of surgery, that is the fact that it can be used concurrently with cataract surgery without the need of an additional surgery that would come with its own risks.
How is the surgery done?
The iStents are implanted with the use of a special lens (gonioprism) which enables the surgeon to visualise the drainage angle of the eye and the trabecular meshwork (TM). This way, 2x or 3x iStents are implanted in the TM. The surgery takes place at a Day Surgery Unit and the patient returns home the same day. It is usually done with local anaesthetic and occasionally sedation.
Efficacy and safety profile:
Retrospective real world data has shown that the eye pressure (IOP) reduces on average by 20% with or without a reduction in the number of glaucoma eye drops used. Risks are similar to those of cataract surgery with a slightly increased risk of a micro bleed in the front of the eye that is almost always self-resolving.
Postoperative Care:
It is the same as with someone having cataract surgery. Post-operative drops are prescribed and should be instilled for 4 weeks following the surgery. The decision on whether to stop any pre-operative glaucoma eye drops is taken on a case by case basis. A post-operative eye pressure (IOP) check should be done on post operative day 1, week 1 and week 4. The patient can return to their usual activities on average 2 weeks after the surgery.
GATT
When is GATT surgery performed?
Clinical studies have demonstrated that the GATT technique is vey effective in Primary Open Angle, Primary Angle Closure as well as Pseudoexfoliative, Pigment Dispersion, Uveitic and Juvenile Glaucomas. The main advantage of this technique is that it is done with an ab-interno approach without affecting the conjunctiva which means that it is a glaucoma surgery which is less invasive, shorter and with quicker recovery surgery that also allows for further glaucoma surgery in the future. This enables the glaucoma specialist to employ stepwise approach in the treatment strategy of a lifelong disease.
At the same time, the GATT technique can be combined with cataract surgery or as a stand alone procedure. The latter makes it an attractive option in secondary glaucomas in younger patients where long term planning is crucial and we usually try to avoid a bleb procedure as a first surgery.
How is the surgery done?
Using a special gonioprism, the surgeon is able to visualise the trabecular meshwork of the eye (TM) and create a 2mm cut in the TM in order to introduce a special micro catheter (like the iTrack™) or suture (Prolene) in the Schlemm’s Canal. Once the catheter has been pushed 180 or 360 degrees within the canal, then using a special technique, the suture or catheter are removed thereby creating a cut through the TM spanning 180 or 360 degrees. This is an effective way of creating a passage for the aqueous fluid to bypass the areas of increased reststance of the TM and allow it to flow into the Schlemm’s canal and then in the systemic circulation. The result of this is a significant lowering The surgery takes place at a Day Surgery Unit and the patient returns home the same day. It is usually done with local anaesthetic and intravenous sedation under anaesthesiology cover.
Efficacy and safety profile:
The GATT technique has consistently shown impressive results with respect to the lowering of intraocular pressure, on average by 9mmHg. It tends to be more effective in secondary glaucomas. It is really important to select carefully the patients that are suitable for this type of surgery. It might not be as effective in patients with very high intraocular pressures on maximum medical treatment or in selected cases of very advanced visual field loss. The rate of sight threatening complications is very low and better than the respective complication rate of traditional glaucoma surgery like the trabeculectomy.
The most common side effects are those of eye pressure spike (IOP) and bleeding in the anterior chamber both of which tend to resolve with medical treatment alone in the majority of cases.
Postoperative Care:It is similar to that of cataract surgery. Post-operative drops are prescribed and should be instilled on average for 4 -8 weeks following the surgery. The decision on whether to stop any pre-operative glaucoma eye drops is taken on a case by case basis. A post-operative eye pressure (IOP) check should be done on post operative day 1, week 1 and then depending on how the eye is healing. The patient can return to their usual activities on average 2 weeks after the surgery but the instructions are tailored to each patient. Weight lifting and strenuous exercise should be avoided for at least 6 weeks after the surgery.
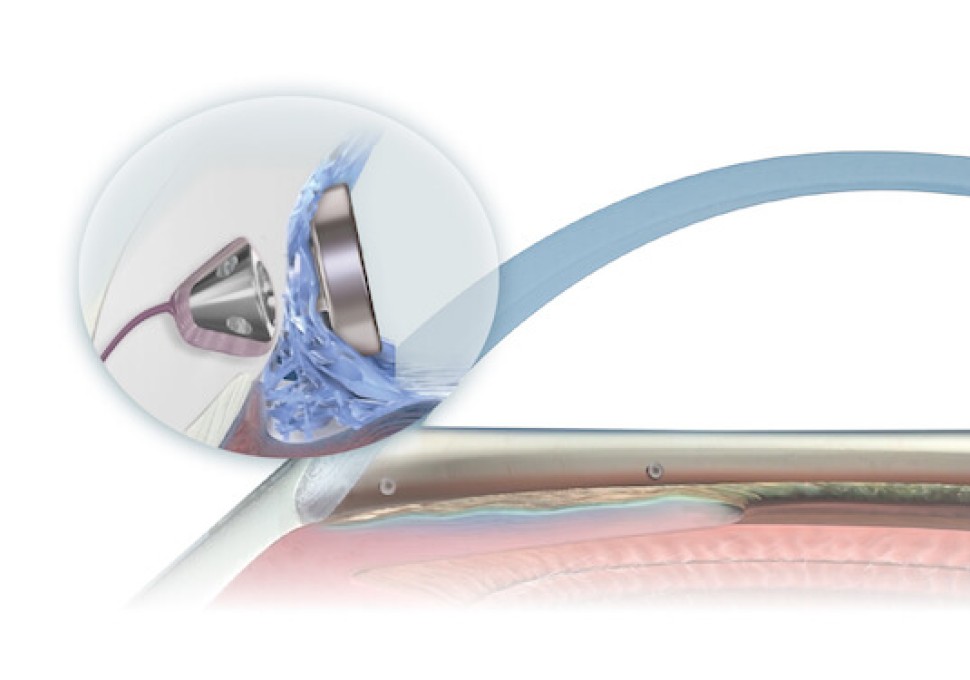
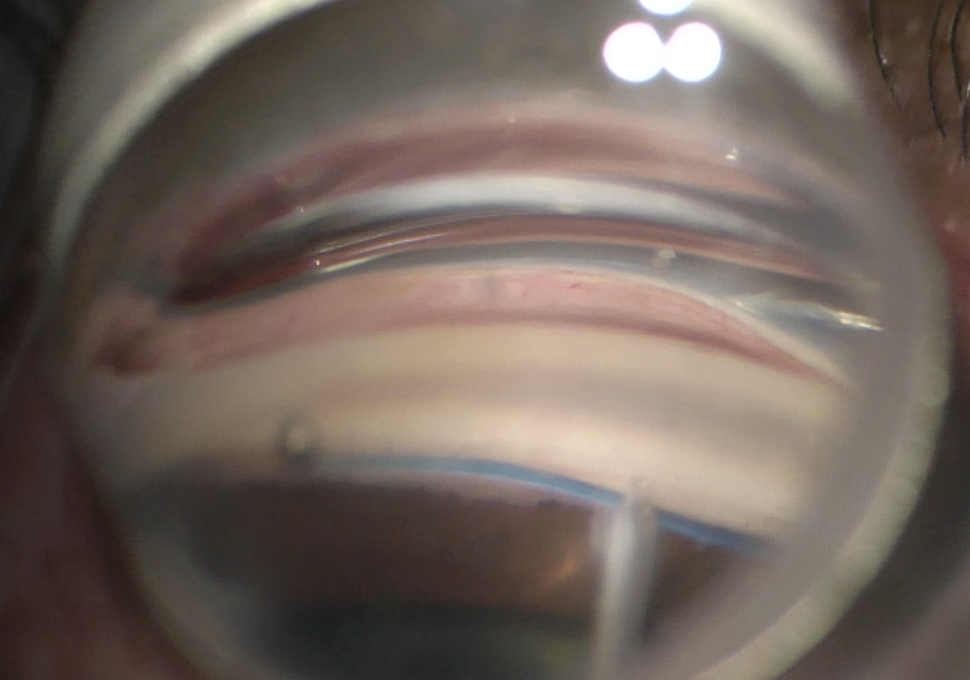
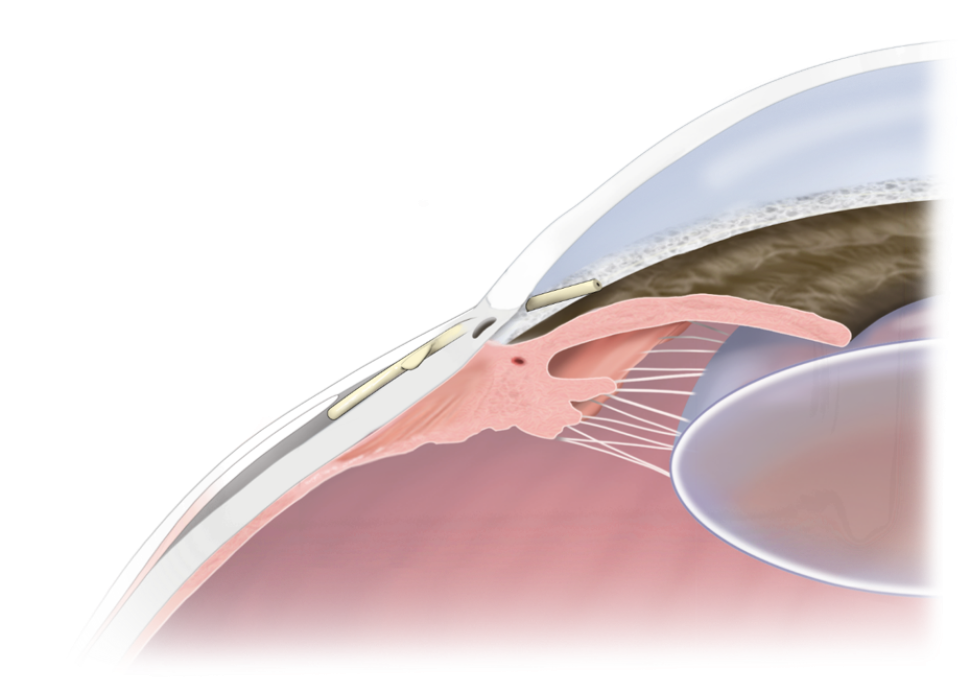
Hydrus
When is this surgery recommended?
The implantation of the Hydrus implant is usually done in combination with cataract surgery in patients who have a symptomatic cataract and a diagnosis of Primary Open Angle Glaucoma (POAG) or Pseudoexfoliative Open Angle Glaucoma. It can also be performed as stand alone surgery.
How is the surgery done?
The surgical technique is similar to the aforementioned techniques of the GATT technique and iStent® implantation. Using a gonioprism, the surgeon visualises the trabecular meshwork and inserts the implant in the Schlemm’s canal with the use of a special injector. The surgery is takes place in a day surgery unit and the patient returns home the same day. It is usually performed with local anaesthesia.
Efficacy and safety profile:
The HORIZON clinical trial is the largest Randomised Control Trial of Microinvasive Glaucoma Surgery (MIGS) and has studied in detail the long term efficacy and safety of the Hydrus® implant. The study looked at patients with mild to moderate POAG that had concurrent cataract surgery and Hydrus® implantation and compared them with patients that had cataract surgery alone (also with mild to moderate POAG). The 2 year results showed that the IOP reduction was 43% greater in the Hydrus group. The 5 year results showed that the patients who underwent combined surgery had a greater chance of a 20% IOP reduction and less chances of needing IOP drops compared to the cataract only group. What is more, the Hydrus implantation together with cataract surgery appears to have a protective effect in visual field preservation and also reduces the risk of additional glaucoma surgery by 50%. The main side effects were transient microhyphema of the anterior chamber (small bleed in the front part of the eye) or transient spike in IOP.
Postoperative Care:
It is the same as with someone having cataract surgery. Post-operative drops are prescribed and should be instilled for 4 weeks following the surgery. The decision on whether to stop any pre-operative glaucoma eye drops is taken on a case by case basis. A post-operative eye pressure (IOP) check should be done on post operative day 1, week 1 and week 4. The patient can return to their usual activities on average 2 weeks after the surgery.
***The implant is currently available for use in the United States, Canada, United Kingdom and some European countries and will be available for use in Greece in the future.
Xen Gel Stent®
When is this surgery recommended?
The Xen Gel Stent® can be used in patients with Primary Open Angle or Primary Angle Closure Glaucoma without peripheral anterior synechiae, Pseudoexfoliative Glaucoma and Pigment Dispersion Glaucoma. Ideally it is done as a stand alone procedure in order to maximise the chances of a successful outcome as cataract surgery can affect its longevity. It is a great option when we are looking to reduce the intraocular pressure effectively while at the same time reduce the surgical risks as it has a better safety profile compared to trabeculectomy.
When compared to trabeculectomy, the Xen Gel Stent® offers some benefits such as reduced risk of developing significant post operative complications related to hypotony, improved bleb morphology and a faster recovery. At the same time, further glaucoma surgery can be done in the future if needed. In terms of potential downsides, the Intraocular Pressure reduction is not as drastic as the one achieved by trabeculectomy but a very low intraocular pressure is needed only for selected patients with very advanced glaucoma.
How is the surgery done?
The surgical techniques vary depending on surgeon’s preference and experience. It can be done ab interno or ab externo - open or closed conjunctiva. The surgery is takes place in a day surgery unit and the patient returns home the same day. It is usually performed with local anaesthesia and sedation under anaesthetic cover.
Efficacy and safety profile:
Regarding the efficacy of the Xen Gel stent, the GPS (Gold-Standard Pathway Study) Randomised Control Trial (RCT) that was published in 2023 and took place across several specialised glaucoma centres across the United States, compared the Xen Gel Stent implantation with the surgery of trabeculectomy in patients diagnosed with open angle glaucoma. 20% of the patients included in the study had advanced disease based on their visual field testing. The study demonstrated that the efficacy of the Xen Gel Stent is similar to that of trabeculectomy at 12 months. Success was defined as the reduction in intraocular pressure without a corresponding increase in the number of glaucoma drops used by the patient. Additionally, the group of the Xen Gel Stent patients had a quicker recovery, less additional post-operative interventions and less post-operative complications and quicker recovery.
Postoperative Care:
Just like any glaucoma surgery that involves the formation of a bleb, the Xen Gel Stent implantation requires close and frequent post-operative follow up especially in the first few weeks after the surgery. Often, additional office based micro-procedures need to be done such as the injection of anti-scarring agents underneath the lining of the eye (subconjunctival 5FU injections) or “needlings”, where any excess scar tissue that impairs the flow of fluid around the implant is displaced improving thus the drainage of aqueous subconjunctivally and reducing the eye pressure. All these procedures are needed in order to increase the long term success of the surgery.
Preserflo™
When is this surgery recommended?
The Preserflo™ microshunt implant is recommended in glaucoma cases where glaucoma eye drops or laser or previous glaucoma surgery have not been succsessful in reducing the eye pressure (IOP) low enough at a level which would reduce the risk of further irreversible visual loss. It can done instead of trabeculectomy in a variety of glaucoma cases. It is suitable for patients with Primary Open Angle or Primary Angle Closure Glaucoma. It can also be used in cases of Pseudoexfoliative Glaucoma, Pigmentary Glaucoma, selected cases of Congenital or Juvenile glaucoma and cases of secondary glaucoma related to raised episcleral pressure like the Sturge Webber Syndrome.
How is the surgery done?
The surgery is done using an open conjunctiva approach. Careful dissection of the conjunctival tissue and Tenons capsule is required as well as meticulous placement of the implant under the Tenons capsule and layered closing of the tissues. Similarly to the surgery of trabeculectomy and Xen Gel Stent implantation, anti-scarring agents like Mitomycin C (MMC) are used in order to improve the changes of achieving good intraocular pressure control over a prolonged period of time. The surgery is takes place in a day surgery unit and the patient returns home the same day. It is usually performed with local anaesthesia and sedation under anaesthetic cover.
Efficacy and safety profile:
Dr Ike Ahmed’s team did a large retrospective review of the clinical outcomes of Preserflo™ microshunt implantation in a heterogenous cohort of glaucoma patients with uncontrolled intraocular pressure. The study showed that the Preserflo™ microshunt had similar success rates with pusblished data for the surgery of Trabeculectomy when looking at the 3 year results. It also showed that this type of surgery offers great IOP reduction while having a more predictable post-operative course with less post-operative procedures being compared to trabeculectomy. This study was published in 2023 and is the largest to date on the subject.
The trial results are in keeping with the personal experience of Dr Siempis of Preserflo who has performed numerous implantations of the Preserflo microshunt in Canada. Some additional benefits of the Preserflo implant over rabeculectomy are the improved morphology of the bleb which is more posterior and located usually in the superonasal conjunctival quadrant, the option of revising the surgery if needed in cases of excess scar tissue around the implant and the ability to perform further filtering surgery in other quadrants of the eye if needed. With respect to the possibility of having corneal issues following the implantation of Preserflo, studies have shown that the chances of this happening are low as long as the tube shunt is correctly positioned more than 600 microns from the corneal endothelium.
Postoperative Care:
Close and frequent post-operative follow up are needed especially in the first few wakes after the surgery. Often, additional office based micro-procedures need to be done like the injection of anti scarring agents underneath the lining of the eye (subconjunctival 5FU injections) or “needlings” where any excess scar tissue that impairs the flow of fluid around the implant is displaced improving thus the drainage of aqueous subconjunctivally and reducing the eye pressure. All these procedures are needed in order to increase the long term success of the surgery. Formal revision surgery in the immediate post-operative period is very uncommon.
***The implant is currently available for use in the United States, Canada, United Kingdom and some European countries and will be available for use in Greece in the future.
Trabeculectomy and Glaucoma Drainage Devices
The operations of Trabeculectomy and Glaucoma Drainage Devices (GDD) implantation have been the mainstay of surgical glaucoma treatment for the past decades. These surgeries are usually performed when medical and/or laser treatment have failed to control the Intraocular Pressure (IOP) or disease progression.
These surgeries are usually very effective in lowering the IOP but there is an increased risk of postoperative complications such as hypotony (low IOP), malignant Glaucoma, bleb leaks, choroidal detachments, infections and more.
For this reason, is is very important that these surgeries are performed by specialised glaucoma surgeons. Dr Siempis has significant surgical experience in the aforementioned surgeries as well as in their postoperative care that is equally crucial with the surgical technique with respect to their long term success in controlling the IOP.
Both the operations trabeculectomy and those of GDD implantation require close follow up in the immediate post operative period in order to manage promptly and effectively any potential complications or to perform additional smaller procedures that would improve the final outcome.
Trabeculectomy
When is this surgery performed?
In some patients, medical or laser treatment of glaucoma are not enough on their own to reduce the IOP at safe levels and prevent further irreversible visual loss. Depending on the type of glaucoma, the age of the patient, the current and target IOP, the specialist could recommend this operation as a next step in order to maintain the remaining vision. The surgery of trabeculectomy, similarly to all glaucoma surgeries, does not improve the vision or reverse any visual loss that has already occurred but can slow down significantly the course of the disease.
How is this surgery done?
The operation takes place in a Day Surgery Unit and the patient usually returns home the same day. It is performed either under sedation and local anaesthetic or under general anaesthetic. The average duration of the surgery is 45 minutes to 1 hour.
The surgery essentially creates a new outflow pathway for the drainage of the aqueous humour, the fluid that is constantly produced and drained within the eye and its impaired drainage is associated with increased IOP and glaucoma. More specifically, a small flap is created in the white part of the eye (sclera) that is constructed in a way that acts like a valve mechanism whose resistance is determined by the placement of special sutures. This flap is covered with the conjunctiva and Tenons capsule which are the natural linings of the eye. The drainage of the aqueous through this flap creates a small transparent “bubble” underneath the eyelid called a “Bleb".
During the surgery, an antiscarring agent called Mitomycin C is used. Mitomycin C has been proven to improve the surgical outcomes by reducing the scar tissue that builds up around the flap/bleb after the surgery as part of the eye’s healing process.
Efficacy and Safety Profile:
All glaucoma surgeries face the body’s natural response for healing and this can determine their long term success. The surgical technique and health of the lining of the eye (conjunctiva) also play an important role on the final outcome. In general, the operation of trabeculectomy can control the IOP in almost 80% of the cases (or more) with or without the use of glaucoma drops in the first year after the surgery. The success rate is additionally determined by factors such as the age of the patient, the race, history of previous glaucoma surgeries and the type of glaucoma.
Just like any intraocular surgery, there is a small but real risk of losing eyesight in the operated eye due to a serious infection or haemorrhage. Other complications include low or high IOP, inflammation, microbleeding, choroidal detachment and most of these can be successfully managed medically.
The surgeon will analyse all the aspects of the surgery during the pre-operative assessment.
Postoperative care:
Trabeculectomy is a high maintenance surgery and requires very close and meticulous follow up in the first few weeks after the surgery. Often, additional smaller in office operations might be needed such as removal of suture with the use of a laser or injections of anti-scarring agents.
Glaucoma Drainage Devices
The Ahmed Glaucoma Valve® (New World Medical), the Baerveldt® tube shunt implant (Johnson and Johnson), the Ahmed Clear Path® (New World Medical), the Molteno® tube shunt (Nove Eye Medical) and most recently the Paul® Glaucoma Implant (PGI, Advanced Ophthalmic Innovations) are the main GDDs that are used worldwide.
The main differences between the devices lie in the size of the plate that is sutured on the sclera (white part of the eye), the diameter of the tube and the presence or absence of a valve mechanism.
Dr Siempis has significant surgical experience in the placement of such devices as well as their postoperative management.
When are these surgeries performed?
These surgeries are usually done when previous glaucoma surgery (mostly in the form of a trabeculectomy in cases of Primary Open Angle or Pseudoexfoliative glaucoma) have failed or as primary surgeries in glaucomas with high risk for surgical failure such as Neovascular Glaucomas, Uveitic Glaucomas, in cases of Anterior Segment Dysgenesis or Previous Corneal Graft Surgery related glaucomas and in Angle Closure Glaucoma with extensive peripheral synechiae.
Other indications for GDD implantation are patients with poor ocular surface or patients over the age of 80 who have more fragile and difficult to handle conjunctiva.
These surgeries do not improve the vision or bring back the vision that has been lost to glaucoma but can slow down significantly the course of the disease in most case and prevent further visual loss.
How are these surgeries performed?
These operation take place in a Day Surgery Unit and the patient usually returns home the same day. They are performed either under sedation and local anaesthetic or under general anaesthetic. The average duration of the surgery is 1 hour and 15 minutes.
A new outflow system is created that constantly drains through a tube the aqueous from the anterior chamber to the subtenons space (under the natural lining of the eye). A patch graft , usually in the form of donated sclera or pericardium (Tutoplast ®), is usually used to cover the tube and reduce the risk of conjunctival breakdown and tube exposure that is a significant risk factor for an infection.
Efficacy and safety profile:
Glaucoma drainage devices have an overall good safety profile, especially the valved ones like the Ahmed Glaucoma Valve® and tend to have a predictable postoperative course in most cases. As far as their efficacy is concerned, studies have shown that they can reduce high intraocular pressures effectively on average to 14-15mmHg on 2.5 glaucoma medications.
Similarly to other glaucoma surgeries, their efficacy can wean off with time due to increased scar tissue formation around them. The success rate in terms of good IOP control can reach 65% at 5 years.
Postoperative care:
Postoperative care differs depending on the type of the device that has been used with the non valved tubes like the Baerveldt device requiring closer post operative follow up.
It is necessary that the patient is seen regularly in the first few weeks after the surgery in order to detect any issues that might arise and require immediate attention either in the form of smaller office based procedures or rarely in the form of another surgery.
Surgical revision of previous glaucoma surgery
Surgical revisions of glaucoma operations are complex and require deep knowledge of the physiology of the surgeries and the causes of failure as well as very careful and meticulous surgical technique at the tissues of eyes that have undergone previous glaucoma surgery are more fragile.
Surgical revision of anterior bleb surgeries (Trabeculectomies, Xen and Preserflo)
Trabeculectomies can some times cause hypotony (low IOP) that in some cases can cause reduction in vision due to maculopathy (Hypotony Maculopathy) or due to extensive detachment of the choroid (the vascular layer of the eye).
These cases could require surgical intervention if the conventional medical management has failed. In such cases, one way of reducing the outflow of fluid and increasing the IOP is to put special compression sutures on the bleb (the area of drainage of the surgery) and in selected cases reverse the operation by patching the scleral flap with sclera or Tutoplast®. If the hypotony is related to a leak from the bleb, then surgical revision of the conjunctival closure might be necessary.
In MIBS surgery with the use of the Xen and Preserflo implants, hypotony is rare as these implants are designed in such a way to minimise the risk of it.
If a Trabeculectomy has stopped functioning due to inadequate drainage of the aqueous, a bleb “needling” can be considered in selected cases to free up any scar tissue and reestablish the flow between the anterior chamber and subconjunctival space. This is usually done in combination with an injection of an antiscarring agent like Mitomycin C.
In MIBS surgeries, “needling” can also be considered in similar cases and if this fails, it is possible to revise the surgery by opening up the conjunctiva, removing any excess scar tissue and at times replacing the implant. This is usually combined with an antiscarring agent injection.
Finally, another reason for revising surgically a trabeculectomy or MIBS operation is if the bleb is causing symptoms of increased discomfort to the patient, a condition called bleb dysesthesia.
Surgical revision of glaucoma drainage devices:
Regarding potential causes for revising a Glaucoma Drainage Device (GDD), the most common one is the exposure of the tube or the plate of the device due to conjunctival breakdown. This is a risk factor for an infection and urgent surgical intervention is needed. In such cases, an attempt is made to cover the area with a patch graft (pericardium or sclera) and healthy adjacent conjunctiva.
Less often, a GDD might need surgical revision due to post operative diplopia or due to inadequate IOP control or due to hypotony.
Contact Us
Dr Siempis accepts new consults at his new private practice in the city centre of Thessaloniki that is located at Mitropoleos 110 Street and is equipped with state of the art diagnostic equipment.
He also accepts new patients at St Luke’s Hospital in Panorama.
Please call +30 2313 022 975 to book an appointment.